|
1
|
- Dr Alan Stewart MRCP
- www.stewartnutrition.co.uk
|
|
2
|
- Some basic concepts
- How deficiencies develop
- Making a nutritional diagnosis
- Simple dietary assessment
- Common health problems: - undernutrition and overnutrition
- Correcting micronutrient deficiencies using BNF listed supplements
|
|
3
|
- Undernutrition
protein-energy – low BMI, malnutrition
anaemia – iron, folate, vitamins B12, B2, C, A and copper
osteoporosis – calcium, vitamin D, physical activity
micronutrient deficiencies - many
- Overnutrition
energy – obesity, high BMI and disease risk
protein (animal) – osteoporosis, renal disease
sodium – high BP/stroke,
heart failure and osteoporosis
micronutrient excess – diet, supplement use or disease
- Poor Food Choices
lack of protective foods – vascular disease, cancer and others
intolerance/allergy – eczema, IBS, migraine, arthritis
foods with therapeutic effects – ginger - migraine, sugar - pain
|
|
4
|
|
|
5
|
|
|
6
|
|
|
7
|
- Protein-energy deficiency
- Anaemia and associated nutrients
- Iron: fatigue and minor symptoms, cardiac and renal failure
- Vitamin B12: neurological health
- Vitamin B1 (alcohol XS): neurological problems/cardiac failure
- Vitamin B2: anaemia and hypertension
- Vitamin C (smoking): increased stroke risk
- Vitamin D: musculo-skeletal health, immunity, major illness
- Zinc: poor growth, reduced immunity, poor wound healing
- Other nutrients: pregnancy, anaemia, immunity, mental health
|
|
8
|
- Movement Bone Fracture
- Respiration Anaemia, muscle fatigue
- Sensitivity Neuropathy,
visual loss, mood
- Nutrition Loss of appetite
- Excretion Liver/Renal Disease
- Reproduction Miscarriage,
NTD pregnancy
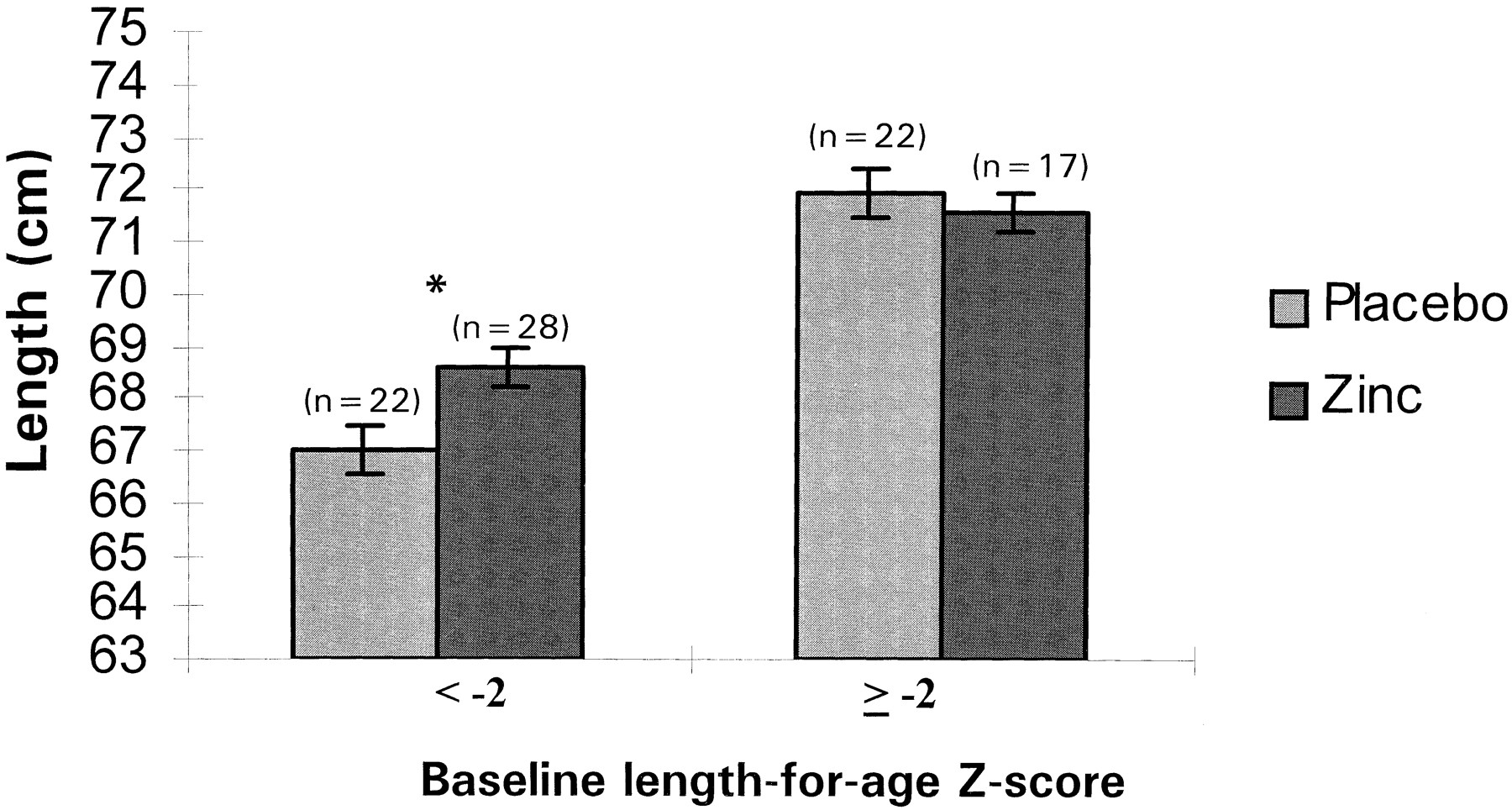
- Growth Low birth weight,
infant stunting
- Defence Infection –
respiratory, GI, GU
|
|
9
|
- Energy (CHO, fats and alcohol): obesity
- Energy-Protein (hospital): re-feeding syndromes - various
- Sugars: dental caries, irritable bowel syndrome, gout
- Animal Protein: gout, osteoporosis, renal disease
- Iron: haemochromatosis, liver disease
- Vitamin A: osteoporosis
- Vitamin A/beta-carotene: cancer risk in smokers and asbestos
- Vitamin B: cancer growth
- Vitamin C: oestrogen metabolism
- Trace element excess: fatigue, CNS problems, poor immunity
|
|
10
|
- Screen all patients to identify those most at risk of being deficient:
- Underweight
- A body mass index (BMI) of less than 18.5kg/m2
- Unintentional Weight Loss
Greater than 10% within the last 3 – 6 months
- or
- Combination of:
- BMI of less than 20kg/m2 and
- Unintentional weight loss >5% within the last 3 – 6 months
- Others at risk:
- Eaten little or nothing (or likely to) for more than 5 days
- Poor absorption, vomiting, high losses, increased need - catabolic
- Already identified with one deficiency e.g. anaemia or osteoporosis
|
|
11
|
- Adequacy
- State of Negative Balance
- Decline in Tissue Stores
- Loss of Function:
1. Symptoms
2. Physical Signs
3. Organ Failure
- Death
Develop over variable amount of time in a recognizable sequence
|
|
12
|
- Adequacy
- State of Negative Balance:
1. Poor Intake Diet + supplements
2. Reduced Absorption Coeliac,
IBD & diet factors
3. Increased Losses
Diarrhoea, menstruation
4. Increased Demand Pregn’cy,
illness + recovery 5. Altered Metabolism Alcohol, drugs, illness, age
genetic factors
- Decline in Tissue Stores
- Loss of Function:
1. Symptoms
2. Physical Signs
3. Organ Failure
- Death
|
|
13
|
- Adequacy
- State of Positive Balance:
1. High Intake Diet + supplements
2. Increased Absorption Haemochromatosis
3. Reduced Losses
Post-menopause
4. Reduced Demand
Elderly
5. Altered Metabolism
Alcohol, drugs, illness, age
genetic factors
- Increase in Tissue Stores
- Loss of Function:
1. Symptoms
2. Physical Signs
3. Organ Failure
- Death
|
|
14
|
- Diet and Nutrition Survey of British Adults (16-64yr)
1986/7
- National Diet and Nutrition Surveys x 4 (1.5 – 85+yr)
1990-2004
- Low Income Diet and Nutrition Survey (1.5 – 85+yr)
2006/7
- NDNS Rolling Programme (1.5 – 85+yr)
2010 - present
- NDNS Young People (6-18 mo)
2013?
|
|
15
|
- Stage Survey Component
- State of Adequacy
- State of Negative Balance
1. Poor intake Diet 4-7 days + Supplement use
2. Reduced absorption
3. Increased losses
4. Increased
requirement
5. Altered
metabolism Alcohol intake
and drugs
- Decline in Tissue Stores Tests
– blood and urine
- Loss of Function:
1. Symptoms NDNS
65+ Depression
2. Physical Signs
BMI, NDNS 4-18 Growth 3.
Organ Failure NDNS 65+
Renal and Liver
- Death NDNS 65+ only
|
|
16
|
- “LRNI – an amount of the nutrient that is enough for only the few people
in a group who have low needs”.
<3% of the population
- Low iron intakes are observed in 33% of women of menstruating age
|
|
17
|
- World Health Organisation Normal Ranges;
1.5-6.0 yrs >11.0g/dl, adult women >12.0g/dl, adult men >13.0g/dl.
- Adult ranges have been adopted from ages 15yrs and upward
- British laboratories often use a normal range of >11.5g/dl for adult
women
- Levels of 11.5-11.9g/dl in women can indicate symptomatic iron
deficiency
|
|
18
|
- Poor Diet Poor Diet Poor Diet
- Reduced Absorption Menstrual Losses GI Blood Loss
- diet – tea/tannins Reduced Absorption Disease/ Unknown
- - disease - diet and disease Mixed Deficiencies
|
|
19
|
- History
- Physical
Examination
- Laboratory
Investigation
|
|
20
|
- History Intake: diet + supplements
Risk Factors for deficiency
Symptoms of deficiency
- Physical Anthropometric Measures
Examination (Body Mass Index - kg/m2)
Signs of Deficiency
Signs of Underlying Disease
- Laboratory Blood and Urine Tests
Investigation Bone Mineral Density
X-Ray
|
|
21
|
- Protein –animal/vegetarian
- Fish and oily fish
- Fruit and Vegetables
- Quality Carbohydrates
- Dairy or quality substitute
- Alcohol
- Salt (sodium)
- Sugar NMES (non-milk extrinsic sugars)
- Fat
|
|
22
|
- Assess by interview and description of typical week-day’s diet or from
dietary questionnaire
- Five Main Food Groups
- Protein –animal/vegetarian
- Fish and oily fish
- Fruit and Vegetables
- Quality Carbohydrates
- Dairy or quality substitute
- Four Main Undesirables
- Alcohol
- Salt (sodium)
- Sugar NMES (non-milk extrinsic sugars)
- Fat
|
|
23
|
- Protein –animal/veget. -
Protein, vit B, Fe, Zn
- Fish - Protein, vit B12, n-3
EFAs
- Fruit and Vegetables - Vit C, K,
Mg, fibre
- Quality Carbohydrate - Energy,
fibre, vit B, Mg
- Dairy or substitute -
Protein, Ca, I2 vit B12, B2 A
- Alcohol <21/14 units/wk Assess
units/week
- Salt (sodium) <6g/day 80%
in savoury food
- Sugar <11% energy 80% in
foods & drinks
- Fat <35% energy Meat, dairy, cakes, pastry biscuits etc
|
|
24
|
- Protein 7 Good Portions/week
- (animal or vegetarian)
- Fish >2
Portions/week
>1 Oily
type/week
- Fruit and Vegetables >5
Portions/day
- Dairy Foods >1.5-2.5
Portions/day
- (or soya substitute)
- Quality Carbohydrate >1-4
Portions/day
- (High Fibre) 12-24g/day
|
|
25
|
- Yes
- Wholegrain (wheat, oat or other) breakfast cereal
- Wholemeal bread
- White bread (UK fortified)
- Fresh potato especially with skin
- Brown rice or brown pasta
- Chappati
- No
- White pasta
- White rice
- Pizza
- Noodles
|
|
26
|
|
|
27
|
|
|
28
|
|
|
29
|
|
|
30
|
|
|
31
|
- Alcohol - 50% exceed safe limits - suspect if:
- overweight especially abdominal obesity
- high blood pressure – uncontrolled
- depression, mood change, insomnia
- abnormal liver function tests
- raised triglycerides
- raised uric acid or gout
- Sugar - 50% of adults exceed target - suspect if:
- overweight especially age <30 yrs
- poor dental health
- poorly controlled diabetic
- lower-socioeconomic group
- non-alcohol consumer
- high intake of sweet foods/added sugar
|
|
32
|
- Salt - 80% of adults exceed target - suspect if:
- high BP
- heart failure
- fluid retention
- high intake of savoury foods/snacks
- Fats - (saturated and trans) 50% exceed - suspect if
- overweight
- high cholesterol or vascular disease
- high intake of meat, processed meat, butter, full-fat
dairy
- high intake of hard margarine cakes, pastry (trans fats)
|
|
33
|
- Protein
- Fish
- Fruit and Vegetables
- Quality Carbohydrate
- Dairy or substitute
- Alcohol
- Salt
- Sugar
- Fat (saturates & trans)
- They provide 60-70% of all micronutrients
- Achieving all targets =
good nutrient intake lower health risks
- But doesn’t guarantee nutritional adequacy
- Displace nutritious foods
- Excessive Intakes =
anti-nutrient effects
increased risk of obesity increased health risks
- Considerable individual variation in effect
|
|
34
|
- Fragile skin
- Poor wound healing
- Apathy
- Wasted muscles
- Poor appetite
- Altered taste sensation
- Impaired swallowing
- Altered bowel habit
- Loose fitting clothes
- Prolonged illness:
chronic infection,
chest disease,
cardiac failure,
cancer etc.
|
|
35
|
- Fragile skin
- Poor wound healing
- Apathy
- Wasted muscles
- Poor appetite
- Altered taste sensation
- Impaired swallowing
- Altered bowel habit
- Loose fitting clothes
- Prolonged illness:
chronic infection,
chest disease,
cardiac failure,
cancer etc.
- Life Stage:
- extremes of age
- adolesence
- pregnant/breastfeeding
- Social Circumstances:
- in receipt of benefits
- living alone – especially men
- Medical History:
- chronic illness/organ failure
- heavy periods
- Family History/Genetic Factors
- Medical Drug Use
- Poor mobility/lack of sun
- Smoking
- Symptoms and Physical Signs
|
|
36
|
- Data from National Diet and
Nutrition Survey British Adults. TSO 2003/4
- <Lower Reference Nutrient Intakes are likely to be adequate for <3%
of the population. Ref: Dietary
Reference Values for Food Energy and Nutrient for the UK. HMSO 1991
|
|
37
|
- Data from National Diet and
Nutrition Survey British Adults. TSO 2003/4
- <Lower Reference Nutrient Intake are likely to be adequate for <3%
of the population. Ref: Dietary
Reference Values for Food Energy and Nutrient for the UK. HMSO 1991
|
|
38
|
- Sample of ~2000 people aged 2 to 85+ yrs
- Household where >1adult in receipt of one or more benefits
- Increased risks of:
- obesity
- physical inactivity
- smoking
- alcohol excess – slightly in women only but not men
- Poorer intakes and status of:
- folate
- vitamin C
- vitamin D
- not iron and anaemia
- Causative factor: more lack of education rather than money
- Dietary solution costs ~ £7:00/week:
fresh potatoes, DGLV – dark green leafy vegetables, fruit, eggs
and tinned oily fish
(see lecture www.stewartnutrition.co.uk for detail)
|
|
39
|
- Both studies assessed new patients, with no clear diagnosis, who were
referred to a medical clinic
- Studies assessed what key element was required to reach the final
diagnosis
- References
Hampton JR et al. BMJ. 1975;2:486-9
Peterson MC et al. West Med J. 1992;156(2):163-5
|
|
40
|
- Heart Disease Prevention (2)
- Coronary Heart Disease (10)
- Heart Failure (4) Lifestyle, vit B1
- Hypertension (3) Lifestyle, vit B2
- Stroke and TIA (8)
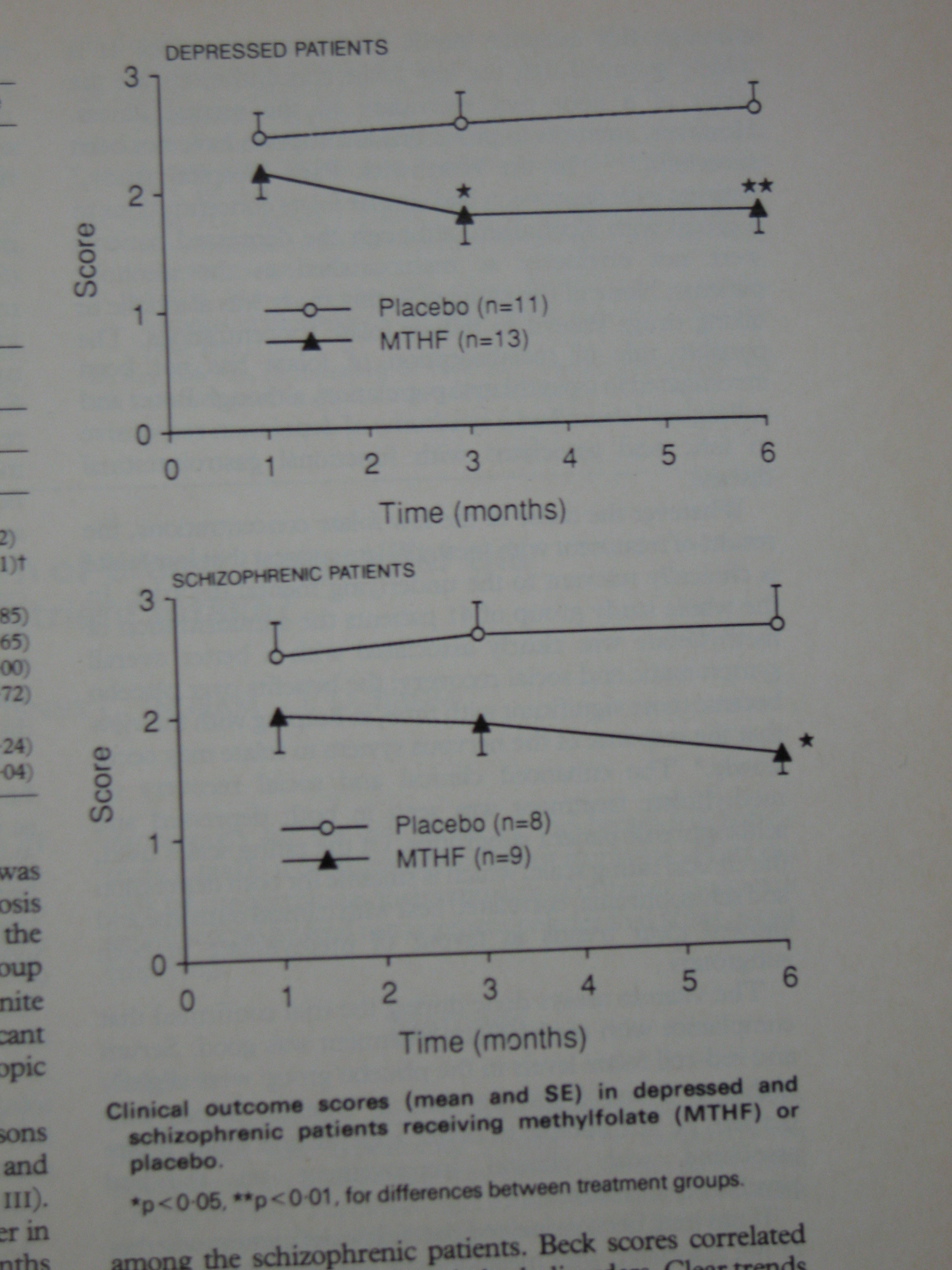
- Depression (3) Folate
- Mental Health (6) Folate
- Dementia (2) Folate + vit B12
- Chronic Kidney Disease (5) Many
- Cancer (2) Caution with vitamins
- Osteoporosis (? in 2013) Ca + vit D, avoid vit A XS
- Maternity (1) Lifestyle, folic acid, vit D
- Child Health Surveillance (1) Healthy diet, surestart, Zn
- Anaemia (0)
- Low BMI/Wt Loss (0)
|
|
41
|
- Sodium restriction if oedema, unintentional wt gain
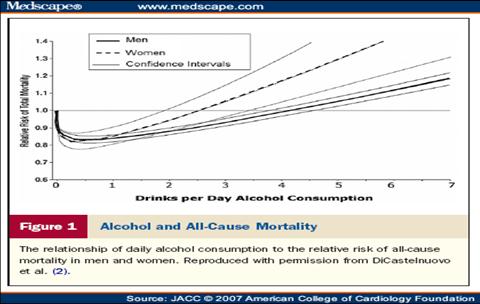
- Alcohol restriction – cardiac depressant
- Optimum weight
- Regular exercise
- Diet – adequate protein, easy to digest,
- Good intakes of K and Mg – potato, vegetable soup
- Correct anaemia and iron deficiency
- Correct thiamin deficiency
|
|
42
|
- Some micronutrient deficiencies are common
- Some nutrients are important for energy production and muscle function
- Thiamin - vit B1, n-3 EFAs, CoQ10, L-carnitine amino acids, taurine, Fe,
K and Mg
- Trials of some show benefit
- Further trials of targeted appropriate nutrition support needed
|
|
43
|
- “Here is one of the fatal forms of heart disease which is curable”
- Foods: bread, meat, breakfast cereals
- Clinical Features:
alcohol XS – CNS effects
peripheral neuropathy
cardiac failure + tachycardia
calf muscle tenderness
- No oral/skin signs
- Test: RBC transketolase activation coefficient
|
|
44
|
- ETKAC - measures the increase in stimulation of a vitamin B1 dependent
enzyme following the addition of vitamin B1 in the laboratory
- A high level ( >1.25) indicates pre-existing biochemical deficiency
- ETKAC was not measured in infants age 1.5 to 4.5 yrs
|
|
45
|
- Address the Cause(s)
very poor diet reliant upon white rice and sugar, alcohol XS,,
persistent vomiting, unintentional weight loss >5%
- Dietary Advice
healthy eating – wholegrain cereals, pork, eggs, fish, nuts
fortified foods – UK white flour/bread, some breakfast cereals
- Supplement with appropriate amounts of nutrient
Severe deficiency (confusion, ataxia, neurological signs, heart
failure) especially if alcohol XS – parenteral injections (BNF)
Mild deficit/poor diet oral B1 25-100ug X 3 /day for >2 months
- Consider need for other nutrients
Assess folate, zinc and other nutrients if alcohol XS, wt loss Many
will also need vit B Co Forte x 3/day or multivitamins
- Once main deficiency corrected
Treat >2 months or until full neurological/cardiac recovery
Many need long-term vit. B (thiamin >5 mg/day) /multivitamin
Caution if cancer especially if rapid growing
|
|
46
|
- 83 patients with three genotypes for MTHFR enzyme (folate metabolism)
- Increased cardiovascular risk homozygous for 677C->T polymorphism
- 31 with TT genotype had higher systolic BP, unresponsive to drug
treatment
- Given riboflavin 1.6 mg/day 2004 & 2008
- Fall in BP
Sys -9.2 + 12.8 mmHg
Dias -6.0 + 9.9 mmH
|
|
47
|
- Several studies in pregnant women and children in developing countries
have shown enhanced response to iron deficiency when riboflavin is given
with iron supplements
- In a trial in Sheffield involving 123 women age 19-25 yrs who were
biochemically riboflavin deficient the three groups received placebo or
2 mg or 4 mg per day for 8 weeks
- Both doses resulted in a modest rise in Hb with a dose-response effect
- Those with the poorest status (found in 20% of UK) experienced a rise of
~0.4g/dl in Hb
- There was no observed increase in iron absorption and improved
mobilisation from tissues is considered a possibility
|
|
48
|
- Address the Cause(s)
poor diet low in dairy foods especially full-fat, alcohol XS,
unintentional weight loss >5%
- Dietary Advice
healthy eating – milk, full-fat cheese, eggs, wholemeal
bread
fortified foods – some breakfast cereals
- Supplement with appropriate amounts of nutrient
No separate supplement use vit.B Co Forte X 3 = 6 mg
Yellow discolouration of urine is expected and harmless
- Consider need for other nutrients
Assess anaemia and iron (reduced absorption)
Dairy-free diet consider calcium + multivit/multimineral
Consider folate, zinc and other nutrients if alcohol XS
- Once main deficiency corrected
Treat >2 months
Clearance of angular stomatitis within 4 weeks is expected
Caution if cancer especially if rapid growing
|
|
49
|
- Redness, cracking and soreness at mouth corners
- Causes:
- nutritional deficiency – iron, riboflavin possibly other B
vits.
- candida or mixed bacterial infection
- poorly fitting dentures or dribbling
- Assessment:
- dietary history
- risk factors for nutrient lack
- unilateral = mechanical; bilateral =
infection/nutritional
- failure to clear with antifungal/bacterial = nutrient
deficiency
- Investigation:
- Full blood count
- other nutrients – iron, folate as indicated, vit B12 in elderly
- Nutritional Treatment
- Vit B Co Forte x 3 per day for 8 weeks and healthy diet
- other supplements as indicated
- expect clearance in 4-8 weeks if not reassess
|
|
50
|
|
|
51
|
|
|
52
|
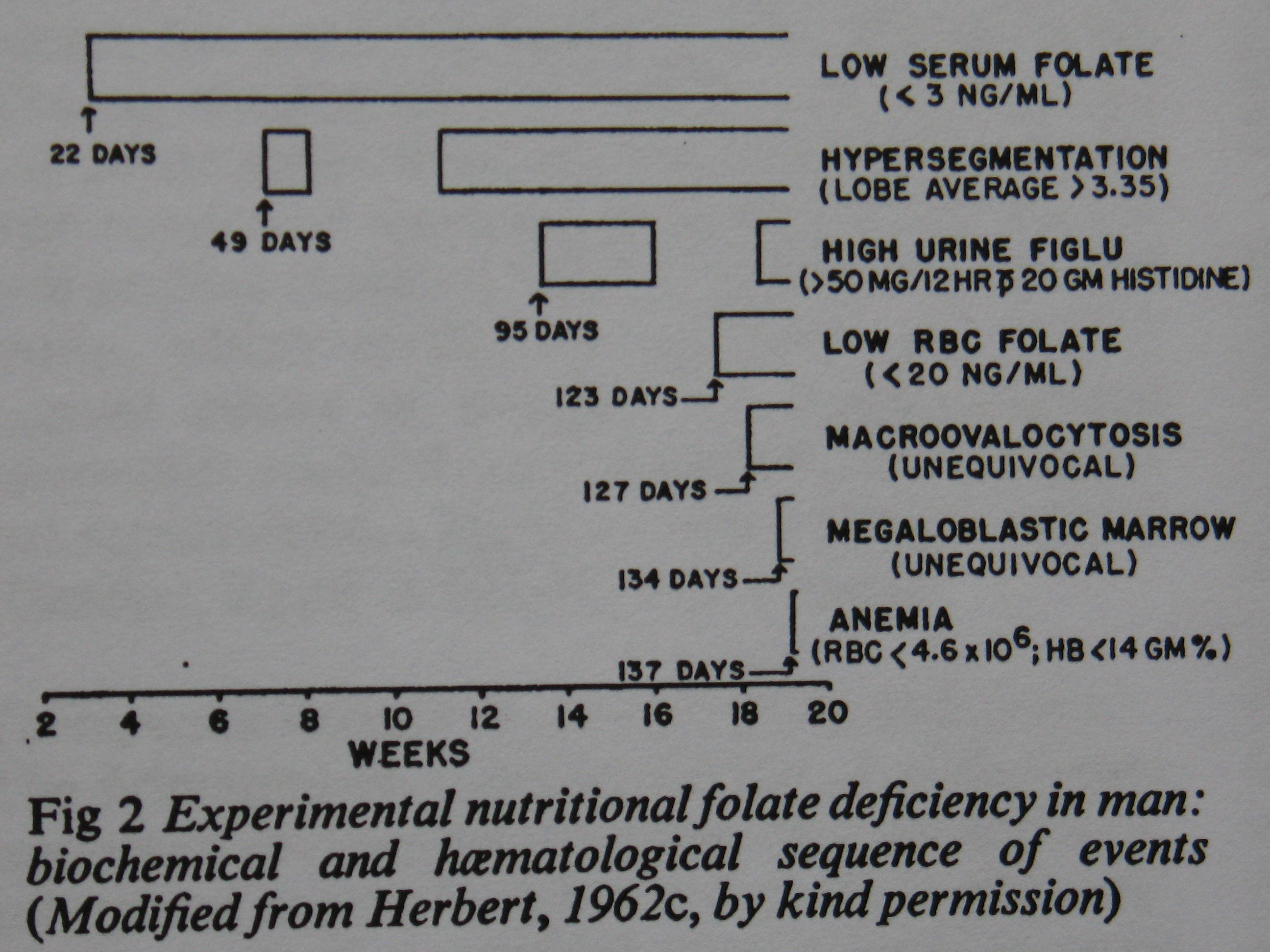
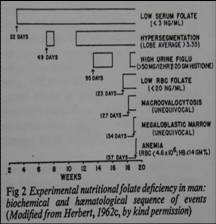
- 35 year old healthy male
All vegetables were triple-boiled in large amount of water
- Intake estimated. <25 ug/day vs. requirement of 200ug/day
- Supplements of all other B vitamins
- 3 weeks – fall in serum folate
- 7 weeks – white cells neutrophil
hypersegmentation
- 16 weeks - depression &
irritability
- 17 weeks - fall in erythrocyte
folate
- 18-20 weeks - macrocytic red blood cells, fall in haemoglobin, bone
marrow – megaloblastic anaemia
|
|
53
|
- The normal ranges for red cell folate and method of analysis varied with
each study;
infants > 400nmol/l, children and adults > 350nmol/l and
the elderly > 345nmol/l
- Folate status is influenced by alcohol excess and altered metabolism in
the elderly
- Pregnant or breast feeding women were excluded from the adult NDNS
|
|
54
|
- Address the Cause(s)
poor diet, alcohol XS, malabsorption, elderly, blood disorders
- Dietary Advice
healthy eating – green leafy vegetables, potatoes, oranges
fortified foods – some breakfast cereals
- Supplement with appropriate amounts of nutrient
Folic acid 5 mg x 1-3/day for proven deficiency; x1/wk if
MTX
Pregnancy 400 ug/day but high NTD risk 5 mg/day (see BNF)
Caution if cancer – may promote tumor growth ask oncologist
- Consider need for other nutrients
Other deficiencies - vitamin B if alcohol, zinc if
malabsorption
poor diet in pregnancy consider prenatal multivit/multimineral
- Once main deficiency corrected
Retest rbc folate (better than serum folate) after 2-3 months
High daily folic acid may reduce zinc absorption long-term
Consider long-term 400ug/day or 5mg/wk if status is poor
|
|
55
|
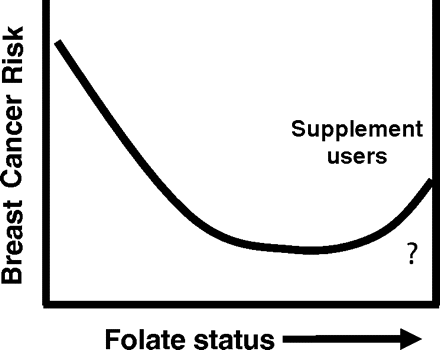
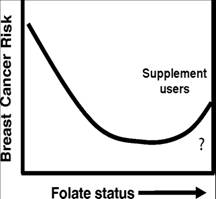
- Low dietary intakes increase the risk of alcohol-associated breast
cancer
- High intakes of folic acid from supplements may increase the growth of
an existing tumor
- High serum vitamin B12 level associated with increased risk of advanced
prostate cancer
Johansson M et al Cancer Epidemiol Biomarkers Prev
2008;17(2):279-85
Hultdin J et al Int J Cancer 2004;113:819-24
- Thiamin - vit B1 is growth-promoting for some cancers
Langbein et al
|
|
56
|
- Cancer Treatment, Herbal and Nutritional Supplements
- Ask patients what they are taking before commencing treatment
- Urge patients to seek professional advice on diet and supplements
- If patients are keen take a good quality one-a-day multivitamin and
mineral; do not exceed the dose
- Antioxidants may reduce the effectiveness of chemotherapy; avoid their
use especially high doses
- Monitor and report any adverse interaction through the Yellow Card
Scheme (www.mhra.gov.uk)
|
|
57
|
- A serum vitamin B12 of 118pmol/l is equivalent to 154pg/ml
- Macrocytosis (MCV >101fl) was seen in: 1-3% of teenagers, 9% of
adults,
2% of free-living elderly and 3% of elderly in institutions.
- Macrocytosis is often due to alcohol excess and not vitamin B12
deficiency
|
|
58
|
- Address the Cause(s)
vegetarian/vegans, malabsorption, poor gastric acid (now the
commonest cause - reduces absorption of food-derived but not
supplemental forms), PPIs, pernicious anaemia - rare
- Dietary Advice
healthy eating – protein, meat, milk, fish, eggs
fortified foods some soya milks b’fast cereals, Flora Proactive
- Supplement with appropriate amounts of nutrient
Parenteral Injections for severe deficiency (signs, anaemia or
mental symptoms) or malabsorption (see NHS Direct)
Mild deficit/poor diet oral B1210-50ug/day - 2 months + retest
- Consider need for other nutrients
Vegetarian/vegans – iron, zinc, calcium: elderly Ca/vit D
- Once main deficiency corrected
Malabsorption/severe deficiency parenterally - 2-3 months
Use multivitamin if poor diet, elderly, some pregnant/lactating
Caution if cancer especially prostate – reassess need
|
|
59
|
- Scurvy is rare and occurs when plasma level is <3umol/l
- Mild deficit, <11 umol/l, may
cause depression and mood change; in the UK 25% of men and 16% of women
with a low income are deficient – Mosdol A et al J Pub Hlth
2008;30:456-60
(see presentation on LIDNS on www.stewartnutrition.co.uk)
- Levels >50 umol occur as a result of eating >5 portions of fruit
and vegetables daily
- Good vitamin C status is associated with a lower risk of:
- heart failure - Pfister R et al Am Ht J. 2011:162:246-53
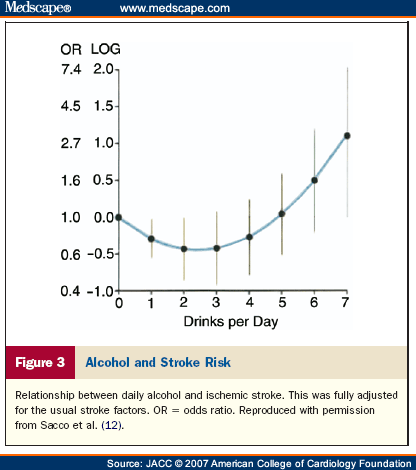
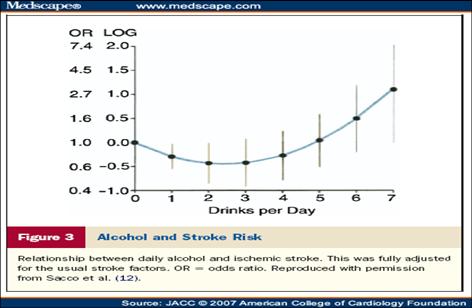
- stroke - Kurl S et al Stroke 2002;33:1568-73
- The results of trials of vitamin C supplements show no reduction in such
diseases but those most at risk of deficit – males, elderly, poor diet,
smokers and lower socio-economic groups were not especially targeted
- Consider assessing status in high risk individuals
|
|
60
|
- Approx. 20% of adults and 12% of the elderly took supplements of vitamin
C
- Approx. 25% of British adults smoke and this declines after the age of
65 years
- Aspirin was taken by 20% of free-living elderly and 24% of
institutionalised elderly
|
|
61
|
- Address the Cause(s)
poor diet – lack of fruit, vegetables, potato and XS of pasta
& rice, poor teeth/chewing, heavy smoking and asprin/NSAIDs
- Dietary Advice
healthy eating – fresh vegetables, fruit/juice, potatoes + skins
- Supplement with appropriate amounts of nutrient
Ascorbic acid 200 – 500 mg/day for 8 weeks
Adverse effects rare: Safe Upper Levels 1000 mg
- Consider need for other nutrients
Anaemia (iron) and folate lack are possible/likely
- Once main deficiency corrected
If healthy diet cannot be guaranteed long term supplement
200mg/day may be needed by a few elderly, heavy smokers High doses may
increase risk of cataract in steroid users, increase breast cancer risk and
rarely oxalate renal stones
(see Safety of Supplements www.stewartnutrition.co.uk )
|
|
62
|
- Normal ranges: infants age
1.5-4.5yrs > 10.0ug/l,
females age >4yrs-adult
> 15.0ug/l, males age
>4yrs-adult > 20.0ug/l
- Plasma ferritin can be elevated by acute or chronic inflammation,
infection or liver disease and is not a reliable measure of iron status
in ill and elderly people
|
|
63
|
- All Hb >12.0g/dl
- Iron Deficient 616
serum ferritin <21ug/l
- Not iron deficient 10,945
- Analysis by Chi squared:
Fatigue p=
0.0026
Irritability p=
0.003
Headache p= 0.0004
- BMJ on line 28/6/2003
Waalen J, Felitti V and Beutler E
|
|
64
|
- Address the Cause(s)
vegetarian/vegan diet, XS tea, heavy periods, GI bleeding
- Dietary Advice
healthy eating – red meat, liver, beans, eggs, green veg;
fortified foods - white bread and some breakfast cereals
- Supplement with appropriate amounts of nutrient
Ferrous Sulphate 200 mg 1-2/day always with fruit/juice
Iron supplements must be taken 2 hrs away from tea/coffee
GI upset likely if dietary advice not followed or high doses
Prolonged use may reduce zinc absorption
- Consider need for other nutrients
Vit B2 lack and rarely vits C, A and copper cause iron lack
Give Vit. B Co Strong x 2/day or Forceval x 1/day as needed
- Once main deficiency corrected
Retest (Hb and ferritin) after 2 months
Continue supplements for 3 months to replenish stores
Chronic menorrhagia -iron x 1/day for 7 days/cycle with period
|
|
65
|
- Prescribable for the treatment of proven deficiencies or their
- prevention in those at significant risk of undernutrition (see BNF)
- Vitamin Tablets
vitamins A, D, C, B1, B3, B2 v. low doses, (no folic
acid/B12)
Based on formulation from 1940s of a free sample from US
govt.
see Bransby ER BMJ 15th Jan 1944 p77.
- Vit B Tablets Compound and Compound Strong
vitamins B1, B2, B3, (B6 – strong only)
- Liquid ABIDEC and DALIVIT drops
vitamins A,D, C and some B suitable for some infants
- Ketovite
tablet - vitamins C, B, E, K; liquid vitamins A, D2
and B12
- Forceval Adult and Junior
RDA amounts of vitamins and trace elements
Useful but avoid in cholestatic liver disease (Mn XS) and caution
in osteoporosis (vit A XS)
|
|
66
|
- Children’s Vitamin Drops
would help address poor vitamin status in infants; does not
contain iron but iron absorption will be enhanced by vitamin C. Daily dose of 5 drops provides:
- vitamin A 233 ug (for growth and immunity)
- vitamin C 20 mg (for bones, immunity and iron)
- vitamin D 7.5 ug (for bones, teeth and immunity)
Take from 6 months until their 4th birthday.
Not needed if consuming 500 ml of formula milk per day
- Vitamins for Women
would help fulfil increased needs in pregnancy. Contains
- folic acid 400 ug (fetal nervous system development)
- vitamin D 10 ug (calcium absorption, skeletal
development)
- vitamin C 70 ug (healthy tissues and aids iron
absorption)
For pregnant women until their child is 1 yr old
|
|
67
|
|
|
68
|
- Retinol – vitamin A Content of Dairy Foods per 100 g:
Whole Milk 55ug Semi
Skimmed Milk 23ug Yakult None
- “No other article can replace milk.
Absence of milk from the diet or inclusion of unfavourably
modified milk is the origin of most serious diseases. By ordering milk, and especially cream
and butter, not only is this terrible eye disease cured – which I
believe will be discovered in every country when it is looked for – but
these dairy products are of the greatest importance for growth and
development and the cure of our greatest infectious disease.”
|
|
69
|
- 219 Institutionalised orphaned boys many of whom were considered to be
below the standard for height and weight despite the diet being
“adequate”
- 41 Boys were given 1 pint of whole pasteurised milk per day
- Additional margarine, sugar and butter were isocaloric
|
|
70
|
|
|
71
|
|
|
72
|
- Infants age 7-120 days in India with bacterial infection (pneumonia,
sepsis, meningitis)
- Rx Antibiotics or Antibiotics + Zn 10 mg/day
- Outcome – treatment failure (change of Ab, intensive care or death)
- Treatment Failure
Antibiotics alone 17%
Antibiotics + Zn 10%
- 44% of babies had serum Zn <9.2 umol/l – marked deficiency
- Similar benefits in other studies in pneumonia and diarrhoea
|
|
73
|
- Address the Cause(s)
vegetarian/vegan diet, alcohol XS, malabsorption, diarrhoea
- Dietary Advice
healthy eating – red meat, cheese, eggs, nuts and seeds
- Supplement with appropriate amounts of nutrient
Zinc Sulphate (Solvazinc 125 mg (45 mg – elemental) 1-3/day after
food away from tea/coffee, bran/chapatti
Children <10kg ½ tablet/day (see BNF)
GI upset more likely if taken on an empty stomach
- Consider need for other nutrients
If malabsorption/underweight consider multivitamins and if
alcohol XS Vit. B Co Strong x 3/day
- Once main deficiency corrected
Reassess/retest after 8 weeks; target plasma Zn >10.0umol/l
Sample protocol follow guidelines www.izincg.org
Prolonged use (>25 mg/day) may cause Cu lack + anaemia
|
|
74
|
- Loss of bone architecture and mass that leads to an increased risk of fracture
- WHO - A bone mineral density measured by DEXA scan that is >2.5 SD
(standard deviations) below the peak BMD in young normal adults in the
lumbar spine or femoral neck, T Score
- Osteopenia 1.5 – 2.5 SD below peak BMD
|
|
75
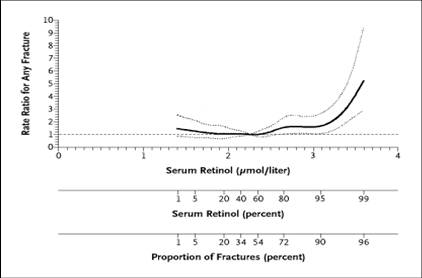
|
- Retinol Total Safe Intake, TSI
= 1500 ug/day
- Risk: Osteoporosis - common
Birth Defects - v. rare
- UK adult diet ~700 ug/day
- Supplements Safe Upper Level
<800 ug/day
none in pregnancy
- High intakes from:
- food – liver, very high dairy
- supplements multivits and CLO
- TSI is exceeded by:
- adults (19-64yrs) 6%
- elderly (65+ yrs) 11%
- Raised Serum Retinol:
- renal impairment
- alcohol excess
- abdominal obesity
|
|
76
|
|
|
77
|
|
|
78
|
- Plasma 25-hydroxyvitamin D levels show considerable seasonal variation
with mild deficiency being commonplace in late winter and spring and
rare in summer
- Dietary sources provide approximately 10% of the body’s content of vitamin D
- Some laboratories adopt a lower end of normal range of 50nmol/l 25-OH D
|
|
79
|
|
|
80
|
- Address the Cause(s)
lack of sun and inactive; diet – lacking eggs/oily fish, obesity,
malabsorption, renal and liver disease
- Dietary Advice
healthy eating – eggs, meat, oily fish: wt loss if obese
fortified foods – margarine, some b’fast cereals and soya milk
- Supplement with appropriate amounts of nutrient
Ca +vit D x 1-2/day for osteoporosis (x2/day if poor diet)
Vit. D 1000 iu (25 ug) OTC x 1-4/day for >3months
Severe deficiency or renal disease parenteral or specialist
supplements (see NHS Direct and
BNF)
Avoid cod liver oil/vitamin A if osteoporosis
- Consider need for other nutrients
Calcium if low intake, young/old or osteoporosis + extra vit D
- Once main deficiency corrected
Re-measure 25OH D after 3-6 months
Target >50 nmol/l but >75 if osteoporosis
Long-term oral vit D 1000 iu/day is safe and suitable for many
|
|
81
|
- Poor grip strength (men)
- Low food/protein intake
- Poor renal function:
raised Pl. HCys and
Retinol
- Raised Hb A1c prediabetes/diabetes
- Inflammatory disease:
raised Pl. copper
(infection, cancer, liver dis)
- Low plasma nutrients:
vit C, Alpha-carotene, B6,
D (men), zinc and selenium
- Not Cholesterol, vit B12, folate, Hb or Beta-carotene
|
|
82
|
- all pregnant or breastfeeding women (vitamin D)
- women trying to conceive and in the first 12 weeks of their pregnancy (folic
acid)
- all children aged 6 months to 5 years (vitamins A, C & D)
- people aged 65 and over (vitamin D)
- people with darker skin or who are not exposed to much sun (vitamin D)
- Those diagnosed with a deficiency by their doctor
|
|
83
|
- Department of Health:
Publish all previous NDNS on line
Clinicians involved in NDNS planning and interpretation
Action group – respond rapidly to NDNS findings
- Education:
Books to include NDNS data
Basic principles to be taught from GCSE to academia
- Clinical Practice:
Targets – for screening for undernutrition in primary care
Dietary assessment – deficiency and excess
Emphasise food-based dietary targets, therapeutic diets
Better availability of tests with clear indications
More appropriate and safer NHS nutritional supplements
|

 Notes
Notes{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}